Needs Assessment Summary
Mayo / NACR SoE Needs Assessments Summaries
Through support by Mayo Clinic’s Spirit of EAGLES program (PI: Kaur, NCI 1U54 CA 153605), NACR and its partners (Southeast American Indian Council and Nebraska Urban Indian Health Coalition) conducted needs assessments of their respective American Indian communities.
Supplemental Documents
Examples of ARS 2013 Items Instruction to Print Reports Blank Navigation Form Offline PT Info Intake Form
What is the purpose of a needs assessment?
- To collect information necessary to design and implement appropriate programs.
- To determine the types of health problems / services currently in existence and those that were “inaccessible” to the community.
- To formulate and implement a culturally competent assessment of specifically targeted populations to collect data regarding the:
- Health needs
- Health-related services being utilized
- Clients’ ability to access services
- Service providers' ability to provide services
Who were the target audiences of the needs assessment?
- American Indians who were:
- Community members living in the specified area
- Recipients of health resources or services in specified area
- Service providers
- High risk populations
- “Selected” populations (e.g., cancer survivors or family members of cancer patients)
- Deaf, blind or disabled
- Infants and children
- Homeless
- Chronically mentally ill
- Developmentally disabled
- Incarcerated and recently released populations
- People who live outside of the core service areas
- People who were identified as “patients” and are receiving little to no care
- Physically and mentally disabled
Why are Needs Assessments Conducted?
- Determines the extent of the problem(s)
- Identifies who is involved with the problem
- Identifies existing resources available to deal with the problem
- Identifies demographic data of population/community involved (e.g., economic status, educational level, religious beliefs, cultural and ethnic background)
- Identifies barriers to providers' ability to develop and implement appropriate programs
- Identifies barriers to clients accessing services and/or complying with medical recommendations
- Reduces personal bias and preferences for program emphasis

Previously, NACR had conducted multiple needs assessments through literature review and one-on-one interviews. The latter were very expensive. Because NACR and its partners needed updated information about their respective communities and monies were limited, the Project Team conducted needs assessments using Audience Response System (ARS) during group activities (convenience sample). The intended population for the study was a convenience sample of a total of 500 adult AI community members, both genders and living within any one of the three geographic settings described above. Participants had to be able to respond to questions posed during the small group sessions; non-English speaking individuals with someone who could translate also could take part. Additionally, while the needs assessment was designed for AIs living within the region, since data collection took place at community events, non-Natives attending the event were welcomed to take part. Each Partner collaborated with local AI organizations to identify and recruit participants at community venues (e.g. health fairs, PowWows, exhibits, education sessions, and community gatherings). The needs assessment facilitator invited all in attendance to take part in a one-to two-hour needs assessment session either during the event or later.
During the sessions, facilitators used Power Point® slides and ARS equipment and software to anonymously collect participants’ responses. After all ARS questions were completed, the facilitator asked the participants for any questions or topics they wanted to discuss. The facilitator returned to the requested questions and the group shared their opinions and discussed how and why the item was important for their local community. The participants also were invited to suggest the types of programs they wanted to have in the future related to the needs assessment topics. The ARS method for collecting needs assessment data during community events was less expensive than one-on-one data collection, more efficient than take-home surveys and for most settings, very successful.
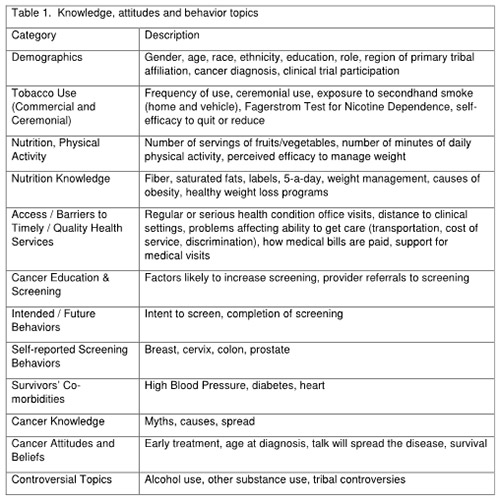
Table 1 summarizes the categories included within the needs assessment.
FINDINGS:

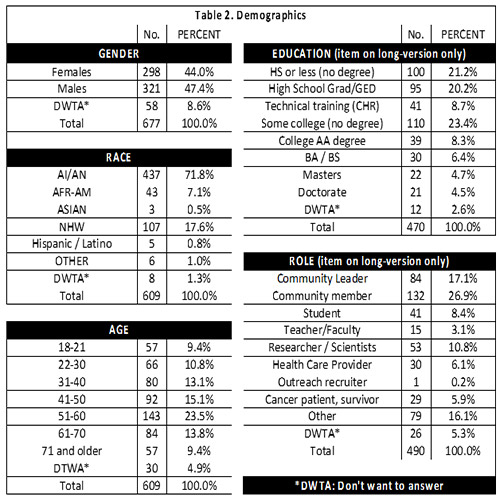
The Partners collected needs assessment data from 677 community members. Examples of findings:
- Cancer education knowledge was low
- Barriers to accessing timely cancer screening and care services were excessive
- Tobacco use was excessive
- Daily physical activity was insufficient for most participants.
AI community members requested:
- More culturally specific and easy-to-understand cancer information
- More stories from AI cancer survivors and their family caregivers
- Access to Native Patient Navigation services
- Access to screening (specifically to FL and GA State recognized tribes – struggle to get on NBCCEDP programs; no access to colon or prostate cancer screenings)
- Their healthcare providers needed more cultural competency training to deal with American Indian patients more respectfully, particularly in the southeast USA.